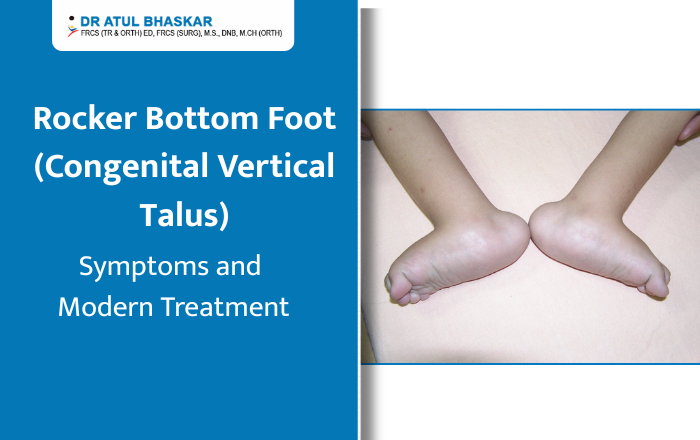
Imagine holding your newborn for the very first time and noticing that one or both of their tiny feet looks unusual — the sole curves outward like the bottom of a rocking chair, and no matter how gently you try to move it, it stays stiff. Your heart sinks. You have questions, and you need answers. If this sounds familiar, you may be looking at a condition called rocker bottom foot, medically known as Congenital Vertical Talus (CVT). It sounds intimidating, but here is the truth — this condition is rare, it is diagnosable, and most importantly, it is very treatable, especially when caught early. This article will walk you through everything you need to know, in plain, simple language. What Is Rocker Bottom Foot? Rocker bottom foot is a congenital (present at birth) deformity where the talus bone in the foot points straight downward instead of sitting at its natural angle. This causes the sole of the foot to bow outward, creating that distinctive rounded, rocker-like shape. Unlike a simple flat foot — which is flexible and often harmless — congenital vertical talus is rigid. The foot cannot be moved into a normal position by hand. It affects roughly 1 in 10,000 newborns and occurs in both feet in about half of all cases. What Causes It? In many children, rocker bottom foot occurs on its own without any clear reason. However, it is sometimes linked to: Neuromuscular conditions like spina bifida or arthrogryposis Chromosomal abnormalities such as Trisomy 13 or Trisomy 18 Connective tissue disorders In some cases, it can even be spotted during a prenatal ultrasound. If your doctor notices something unusual before birth, early referral to a pediatric orthopedic specialist is strongly recommended. Symptoms: What Should You Look For? Spotting congenital vertical talus early makes a significant difference in how smoothly treatment goes. Here are the key signs: The sole of the foot is visibly rounded or convex — like the underside of a rocking chair The foot feels stiff and rigid, even when you try to gently flex it The heel points downward while the front of the foot turns upward and outward There may be a bony bump visible on the inner side of the foot Standard baby shoes or booties simply do not fit properly As the child grows older and begins to walk, untreated rocker bottom foot can cause limping, pain, and the development of thick calluses on the curved sole of the foot. How Is It Diagnosed? A pediatric orthopedic surgeon will first perform a careful physical examination, checking how the foot moves and feels. They will then use X-rays — including stress-position views — to confirm the vertical position of the talus bone and rule out other conditions like flexible flatfoot or oblique talus. The earlier the diagnosis, the better. Babies diagnosed before 6 months of age respond far better to non-surgical treatment because their joints and soft tissues are still highly flexible. Modern Treatment Options for Rocker Bottom Foot The Dobbs Casting Method The biggest shift in congenital vertical talus treatment over the past two decades has been the Dobbs casting technique. Before this method, surgery was almost always the first option. Today, it is the gold standard first-line approach worldwide. Here is how it works: The surgeon gently manipulates the foot into a better position during each clinic visit, then applies a series of plaster casts — typically over 4 to 6 weeks — to gradually move the bones toward their correct alignment. Studies show this approach achieves meaningful correction in up to 70–80% of cases. After casting, a small procedure under anesthesia — a percutaneous pin fixation — is usually performed to hold the talus in place. This is far less involved than traditional open surgery and carries a much shorter recovery time. When Surgery Is Needed For older children, more severe cases, or situations where casting alone has not achieved full correction, surgical correction may be recommended. This typically involves tendon lengthening and stabilization of the joint, and is most effective when performed between 6 and 18 months of age. After Treatment: Bracing and Follow-Up Treatment does not stop after casting or surgery. Children are placed in a foot abduction brace — similar to what is used after clubfoot treatment — to maintain the corrected position during growth. Physiotherapy exercises also help strengthen the foot muscles over time. Regular follow-ups every six months through the growing years are essential to catch any signs of recurrence early. What Happens If It Goes Untreated? This is important for every parent to understand. Rocker bottom foot does not resolve on its own. Without treatment, children grow up with a painful, rigid deformity that makes walking difficult, limits physical activity, and may eventually require far more complex surgery in adulthood. Early action is not optional — it is everything. Trust Your Child’s Feet to the Right Hands If you suspect your child has rocker bottom foot or congenital vertical talus, do not wait. In Mumbai, Dr. Atul Bhaskar, a Pediatric Orthopedic Surgeon with over 33+ years of experience, has helped countless families navigate this condition with skill and compassion. From diagnosis through recovery, Dr. Bhaskar’s approach puts your child’s long-term mobility and quality of life first. Name – Dr. Atul R Bhaskar . PAEDIATRIC ORTHOPAEDIC SURGEON Address: B Wing, Laxmi Business Park, Room No. 114, Sab T V – Kalinga Ln, off New Link Road, Laxmi Industrial Estate, Suresh Nagar, Andheri West, Mumbai, Maharashtra 400053 Phone: 98216 22992 Book a consultation with Dr. Atul Bhaskar today — because every child deserves to walk, run, and play without limits.
Limping in Children: Causes, Diagnosis, and When to Worry
If you’ve noticed your child limping lately, you’re probably worried. And that’s completely normal. As a parent, watching your child walk differently — dragging one leg, favouring one side, or wincing with each step — is unsettling. But here’s the reassuring truth: limping in children is more common than most parents realise, and many causes are simple and treatable. That said, some causes do need urgent attention. This blog will walk you through everything you need to know — from common reasons to serious warning signs — so you can make the right call at the right time. Why Is My Child Limping? Understanding the Basics A limp in a child simply means their walking pattern has changed. It can happen because of pain, weakness, or a structural problem in the leg, hip, knee, or foot. Doctors broadly classify limps into three types — pain-related (antalgic), weakness-related (Trendelenburg), or mechanical (like a leg length difference).Age plays a big role too. A limping toddler is often looked at differently than a limping teenager, because different conditions tend to show up at different stages of development. 9 Most Common Causes of Limping in Children 1. Transient Synovitis — The Most Frequent CulpritThis is the single most common reason for limping in children aged 3–10. It’s a temporary inflammation of the hip joint, often following a cold or viral infection. The good news? It usually gets better on its own within 1–4 weeks with rest.2. Injury or TraumaSprains, minor fractures, or muscle pulls are obvious causes. One commonly missed injury is “toddler’s fracture” — a small crack in the shin bone that can happen even without a noticeable fall.3. Legg-Calve-Perthes (LCP) DiseaseIn this condition, the blood supply to the ball of the hip joint is temporarily disrupted, causing the bone to weaken. It affects about 1 in 1,200 children, mostly boys between 4–10 years. A child limping without pain is often the first — and only — sign.4. Septic Arthritis — A Medical EmergencyThis is a bacterial infection inside a joint. If your child is limping with a fever, refuses to move their leg, and is in severe pain — go to the emergency room immediately. Septic arthritis can permanently damage a joint within hours if not treated.5. Slipped Capital Femoral Epiphysis (SCFE)This condition affects teenagers, particularly overweight boys. The “ball” of the hip slips off its normal position. Many children with SCFE complain of knee pain — but the real problem is in the hip. Surgery is almost always needed.6. Growing Pains vs. Juvenile ArthritisTrue growing pains cause nighttime aching in both legs and do not cause a limp. If your child is limping, has joint swelling, or feels stiff in the mornings for more than 6 weeks, juvenile arthritis should be evaluated.7. Flat Feet or Hip DysplasiaThese structural conditions often cause a painless limp in young children and are frequently missed. Early detection makes treatment far simpler.8. Osteomyelitis (Bone Infection)Similar to septic arthritis, this is a bone infection that causes fever, localised bone pain, and reluctance to walk. It needs prompt treatment with antibiotics or surgery.9. Rare but Serious: Bone Tumors and LeukemiaA persistent child limping — especially with night pain, fatigue, or unexplained weight loss — should never be ignored. Bone pain is a presenting symptom in roughly 25% of childhood leukemia cases. This is rare, but worth ruling out. 7 Red Flag Warning Signs You Should Never Ignore Do not wait. Contact your doctor immediately if your limping child shows any of these signs: Fever along with a limp — possible joint or bone infection Refusal to bear any weight on the leg Swollen, red, or warm joint Limp lasting more than 1–2 weeks Night pain that wakes the child from sleep Unexplained tiredness or weight loss Any limp in an infant or newborn — always abnormal How Do Doctors Diagnose the Cause of a Limp? When you bring your limping child to a doctor, here’s what typically happens: Physical examination comes first. The doctor watches your child walk, checks the range of motion in the hip and knee, looks for swelling, and compares leg lengths. Investigations are chosen based on what’s suspected. X-rays pick up fractures, LCP disease, and SCFE. An ultrasound can detect fluid in the hip joint — a key difference between harmless transient synovitis and dangerous septic arthritis. Blood tests (CRP, ESR, white blood cell count) check for infection or inflammation. An MRI is used when soft tissue or early avascular necrosis needs to be assessed. Doctors also use the Kocher Criteria — four clinical markers — to quickly identify children at high risk for septic arthritis. The more criteria a child meets, the greater the urgency. Treatment: From Rest to Surgery Treatment depends entirely on the cause. Rest and medication work well for transient synovitis and minor injuries — most children recover fully at home. Physiotherapy and bracing help with flat feet, mild hip dysplasia, and certain stages of LCP disease. Surgery becomes necessary for SCFE, severe LCP disease, septic arthritis (joint drainage), and untreated hip dysplasia. The earlier surgery is done when needed, the better the outcome for the growing joint. Special Scenarios Parents Often Search For My child limps only in the morning — Morning stiffness lasting more than 30 minutes alongside a limp in a child points toward juvenile idiopathic arthritis. My child limps after sports — This often suggests stress fractures or Osgood-Schlatter disease in active teenagers. My child limps but doesn’t complain of pain — A painless limp is a structural clue, not a reassuring one. Conditions like LCP disease and hip dysplasia are often completely painless in the early stages. My toddler just started limping — Could be a toddler’s fracture, hip dysplasia, or early transient synovitis. Always worth a check-up. FAQs: Limping in Children Should I go to the ER if my child is limping?Yes — if there is fever, refusal to walk, or a swollen joint. For a mild limp with no other symptoms, a doctor visit within

What Is a Greenstick Fracture in Children? Signs, Treatment & Healing Time
Your child was playing outside, tripped, and landed awkwardly — now they’re crying and holding their arm. You rush over, expecting the worst, but there’s no obvious break. Could it still be a fracture? Yes, it absolutely could. It might be a greenstick fracture — one of the most common yet misunderstood bone injuries in children. As a parent, understanding what a greenstick fracture in children is, how to spot it early, and what treatment looks like can save your child from unnecessary pain and complications. Let’s break it all down in simple, clear terms. What Is a Greenstick Fracture? A greenstick fracture is an incomplete bone break where the bone bends and cracks on one side but doesn’t break all the way through. Picture trying to snap a fresh green twig — it bends and splits rather than breaking cleanly. That’s exactly what happens inside your child’s bone. This type of fracture happens almost exclusively in children because kids’ bones are softer and more flexible than adult bones. The younger the child, the more pliable their bones — which is why greenstick fractures are most common in children under 10 years of age. Where Do Greenstick Fractures Usually Occur? The most common locations include: Forearm (most frequent — from falling on an outstretched hand) Collarbone (clavicle) Shinbone (tibia) Upper arm (humerus) Signs and Symptoms — How Do You Know? Because the bone doesn’t fully snap, a greenstick fracture can easily be mistaken for a sprain. Here’s what to look for: Pain at the injury site, especially when touched Swelling around the affected area Mild bowing or bending of the limb — it may look slightly off Bruising appearing within 24–48 hours Child refusing to use the arm or leg — a classic warning sign in young kids Tenderness that doesn’t improve after a few hours When Should You See a Doctor Immediately? Take your child to a doctor right away if: The limb looks visibly bent or deformed There is severe, continuous pain Fingers or toes below the injury feel numb or look pale or bluish Your child completely refuses to walk (for leg injuries) Never assume it’s just a sprain. In growing children, untreated fractures can affect long-term bone development. How Is a Greenstick Fracture Diagnosed? A doctor will first do a physical examination — checking for swelling, tenderness, and movement. An X-ray is then used to confirm the greenstick fracture diagnosis. In some cases, two different angled X-ray views are needed because the fracture line can be very subtle. Rarely, an MRI may be ordered if the fracture is near a growth plate. Greenstick Fracture Treatment — What to Expect The good news is that most greenstick fractures heal without surgery. Treatment depends on how much the bone has bent. 1. Casting A plaster or fibreglass cast is the most common treatment. It holds the bone still while it heals and prevents the bend from getting worse. Most children wear a cast for 4 to 8 weeks. 2. Splinting For mild cases, a splint may be used initially — especially while swelling is still present — before a proper cast is applied. 3. Realignment (Closed Reduction) If the bone is bent more than 15–20 degrees, the doctor will gently straighten it before casting. This is done under sedation so your child feels no pain during the process. 4. Surgery Surgery is rarely needed for greenstick fractures. It is only considered in very severe cases where the bone cannot be properly aligned otherwise. At-Home Care Tips Elevate the injured limb for the first 48 hours Use an ice pack (wrapped in cloth) for 15–20 minutes at a time Give pain relief as directed by your doctor Keep the cast completely dry Greenstick Fracture Healing Time Children’s bones heal much faster than adults’ because they are still actively growing. Here’s a simple guide: Child’s Age Healing Time Under 2 years 3–4 weeks 2–5 years 4–6 weeks 6–10 years 6–8 weeks 10+ years 8–12 weeks After the cast comes off, mild stiffness and weakness are completely normal. Most children return to sports and full activity within 2–4 weeks after cast removal. FAQ Q1. Can a child walk with a greenstick fracture? If the fracture is in the leg, some walking may be possible — but it can make the injury worse. Always get an X-ray before letting your child put weight on an injured leg. Q2. Does a greenstick fracture need a cast? Almost always, yes. Without a cast, the bone can bow further or heal in a bent position, causing long-term issues. Q3. Will it affect my child’s bone growth? When diagnosed and treated on time, it typically does not affect growth. However, if the growth plate is involved, your doctor will monitor the healing closely. Trust Your Child’s Recovery to the Right Hands A greenstick fracture may sound less serious than a full break — but it is still a real fracture that needs proper treatment. Catching it early and treating it correctly makes all the difference. Dr. Atul Bhaskar — Paediatric Orthopaedic Surgeon, Mumbai When it comes to your child’s bones, you want a doctor who has seen it all — and treated it all. Dr. Atul Bhaskar is one of Mumbai’s most trusted Paediatric Orthopaedic Surgeons with 33+ years of experience treating children’s bone injuries, including greenstick fractures. Families across Mumbai rely on Dr. Bhaskar for his calm, child-friendly approach and his deep knowledge of growing bones. ✅ 33+ years in paediatric orthopaedics ✅ Thousands of successful fracture treatments in children ✅ Gentle, child-friendly approach ✅ Trusted by Mumbai families for over three decades Your child’s bones are still growing — make sure they heal right. Book a consultation with Dr. Atul Bhaskar today and give your child the care their recovery truly deserves.

Delayed Walking in Toddlers: Causes, Signs & Treatment
You dressed them up, you cheered them on, and you waited. But while other toddlers at the park are wobbling around on two feet, your little one is still crawling — and that quiet worry in the back of your mind is getting louder. First, take a breath. Delayed walking in toddlers is more common than most parents realize, and in many cases, it is completely treatable. This article will walk you through everything you need to know — from causes and warning signs to treatment options — so you can make the best decision for your child. What Age Should Toddlers Start Walking? Most babies take their first steps somewhere between 9 and 12 months and are walking confidently by 14 to 15 months. The medical community considers 18 months the upper limit of the normal range. If your child is not walking by 18 months, that is the point where a specialist visit becomes important — not a reason to panic, but definitely a reason to act. 7 Common Causes of Delayed Walking in Toddlers Understanding why delayed walking in toddlers happens is the first step toward finding the right solution. 1. Low Muscle Tone (Hypotonia) Some children are born with weaker muscle tone, making it harder to bear weight on their legs. You may notice floppy limbs or difficulty sitting upright for long periods. 2. Hip Dysplasia This is a condition where the hip joint does not form correctly, making it painful or difficult for a toddler to stand and walk. It is one of the most commonly missed causes of walking delay in babies and needs early orthopedic attention. 3. Club Foot or Flat Feet Structural problems in the foot — such as club foot or severely flat feet — can affect balance and make walking uncomfortable. Most of these conditions respond very well to early treatment. 4. Neurological Conditions Conditions like cerebral palsy or spina bifida can affect the brain’s ability to send signals to the muscles. Toddlers with delayed walking due to neurological causes benefit greatly from early diagnosis. 5. Vitamin D Deficiency & Rickets This is surprisingly common in India, especially in cities where children spend less time outdoors. Soft or weak bones caused by Vitamin D deficiency can directly delay a child’s ability to walk. 6. Developmental Coordination Disorder Some children struggle with coordination between the brain and body. Their muscles are fine, but the communication between the two needs support through therapy. 7. Environmental Factors Too much time in a pram or baby walker, and not enough floor time, can slow down natural motor development. The American Academy of Pediatrics (AAP) strongly advises against baby walkers as they can actually delay independent walking. Warning Signs You Should Not Ignore Not every late walker has a medical problem — but certain signs deserve prompt attention: Your toddler is not walking by 18 months They walk only on their toes after 24 months One leg appears stronger or more active than the other Their legs seem unusually stiff or unusually floppy They had started showing signs of walking but then stopped progressing If you notice any of the above, do not wait to “see how it goes.” Early evaluation makes a real difference in outcomes. How Is Walking Delay Diagnosed? A pediatric orthopedic surgeon will typically begin with a physical examination — checking muscle tone, joint flexibility, leg symmetry, and reflexes. Depending on the findings, they may recommend: X-rays to check for hip dysplasia or bone abnormalities Blood tests to check Vitamin D and calcium levels MRI scans if a neurological cause is suspected The goal is to identify the root cause so that treatment targets the right problem. Treatment Options for Delayed Walking in Toddlers Most causes of delayed walking in toddlers are treatable — especially when caught early. Physiotherapy This is often the first line of treatment. A trained physiotherapist uses play-based exercises to strengthen your child’s legs, hips, and core. Most children respond well and begin making visible progress within weeks. Orthotic Devices For children with flat feet or balance issues, supportive footwear or ankle-foot orthotics (AFOs) can provide the stability they need to walk with confidence. Nutritional Treatment If Vitamin D deficiency is the cause, targeted supplementation often leads to quick and noticeable improvement in strength and movement. Surgery — Only When Truly Needed In cases like hip dysplasia or club foot that have not responded to other treatments, surgical correction may be recommended. Modern techniques are safe, and recovery with proper physiotherapy is usually smooth. Take the First Step — Consult Dr. Atul Bhaskar If your child is showing signs of delayed walking, do not wait and wonder. Every month matters when it comes to a growing child’s development. Dr. Atul Bhaskar, Pediatric Orthopedic Surgeon based in Andheri West, Mumbai, brings over 33+ years of experience in diagnosing and treating walking delays, hip dysplasia, club foot, and other pediatric bone and joint conditions. Families across Mumbai trust Dr. Bhaskar for his clear, honest guidance and genuine care for every child he sees. 📍 Andheri West, Mumbai 👨⚕️ 33+ Years | Pediatric Orthopedic Surgery 👉 Book a consultation with Dr. Atul Bhaskar today — because your child deserves to run, jump, and play without limits.

ACL Injuries in Children: Symptoms, Treatment & Recovery
If your child suddenly grabs their knee during a soccer game or basketball practice, your heart might skip a beat. Knee injuries are scary, especially when they happen to our little ones. One of the most common serious knee injuries in young athletes is an ACL injury in children. The ACL, or Anterior Cruciate Ligament, is a strong band of tissue that keeps the knee stable. When it tears, it can sideline your child from sports and cause real pain. The good news? With the right care and treatment, most kids recover well and get back to doing what they love. In this guide, we’ll walk you through everything you need to know about pediatric ACL tears—from spotting the signs to understanding treatment options and helping your child heal. What Is an ACL Injury? The ACL is one of four main ligaments in the knee. It connects the thigh bone to the shin bone and stops the shin from sliding too far forward. It also helps keep your knee stable when you twist or turn. ACL injuries in children are becoming more common than they used to be. More kids are playing competitive sports year-round, which means more chances for injury. Sports like soccer, basketball, football, and gymnastics carry the highest risk. Children’s knees are different from adult knees because they’re still growing. They have growth plates—areas of developing bone tissue near the ends of long bones. This means doctors must be extra careful when treating pediatric ACL injuries to protect normal growth. How Do ACL Injuries Happen in Kids? ACL tears in children usually happen during sports or active play. Common causes include: Suddenly stopping or changing direction while running Landing awkwardly from a jump Getting hit directly on the knee Pivoting with the foot planted firmly on the ground Girls are at higher risk than boys for ACL injuries. This might be due to differences in muscle strength, knee alignment, and how they land from jumps. Kids who specialize in just one sport at a young age or who play on multiple teams may also face higher injury risks due to overuse and fatigue. Recognizing ACL Injury Symptoms in Your Child How do you know if your child has an ACL tear? Watch for these warning signs: Right after the injury: A popping sound or sensation in the knee Sudden, severe pain Rapid swelling (usually within 2-12 hours) Trouble putting weight on the leg Feeling like the knee is unstable or “giving out” In the days following: Ongoing knee pain Difficulty walking, especially on stairs Limited knee movement Continued swelling Not wanting to run or play If your child shows these symptoms after a knee injury, schedule an appointment with a doctor soon. Early diagnosis helps protect the knee from further damage. How Doctors Diagnose ACL Injuries When you visit the doctor, they’ll examine your child’s knee, checking for swelling, tenderness, and stability. They may perform special tests by gently moving the knee in different directions. An MRI scan is usually needed to confirm an ACL tear in children. This imaging test shows a clear picture of the ligament and reveals if there’s any other damage to the knee. X-rays might also be taken to check for broken bones and to see how much your child’s bones have grown. Treatment Options for Pediatric ACL Injuries Treatment depends on several factors: your child’s age, how active they are, and how severe the injury is. Non-Surgical Treatment Some children, especially younger ones or those with partial tears, may not need surgery right away. Non-surgical treatment includes: Rest and activity modification Physical therapy to strengthen the muscles around the knee Wearing a knee brace for support Avoiding sports that involve cutting, pivoting, or jumping The challenge is that a torn ACL doesn’t heal on its own. Without surgery, the knee may remain unstable, which can lead to more damage over time. Surgical Treatment For active kids who want to return to sports, ACL surgery is often recommended. The concern with younger children is protecting their growth plates during surgery. Today, surgeons use special techniques designed for growing kids. These methods reconstruct the ACL while avoiding or minimizing impact on growth plates. The surgery typically uses a graft (tissue taken from another part of the body or from a donor) to rebuild the torn ligament. Surgery for ACL injuries in children is usually done as an outpatient procedure, meaning your child can go home the same day. Recovery Timeline: What to Expect ACL recovery in children takes time and patience. Here’s a general timeline: Weeks 1-6: Focus on reducing swelling and pain. Your child will work on gentle knee movements and may use crutches. Weight-bearing increases gradually. Months 2-4: Physical therapy intensifies. Your child will do exercises to strengthen the leg muscles, improve balance, and increase flexibility. Months 4-9: Sport-specific training begins. Running, jumping, and agility drills are introduced carefully under supervision. Months 9-12: Most children can return to competitive sports around 9-12 months after surgery, once they pass specific strength and function tests. Every child heals at their own pace. Rushing back too soon increases the risk of re-injuring the knee. The Role of Physical Therapy Physical therapy is the backbone of ACL recovery. A good PT program helps your child regain strength, flexibility, and confidence. The therapist will guide your child through exercises that gradually rebuild the knee’s function. As a parent, your encouragement matters. Recovery is long, and kids can get frustrated. Celebrate small victories and remind them that taking time to heal properly means they can play safely for years to come. Can You Prevent ACL Injuries? While you can’t prevent every injury, you can reduce the risk: Enroll your child in training programs that teach proper jumping and landing techniques Make sure they do strength exercises for the legs, hips, and core Encourage rest days and playing multiple sports instead of specializing too early Ensure coaches prioritize safety and proper form Finding the Right Care for
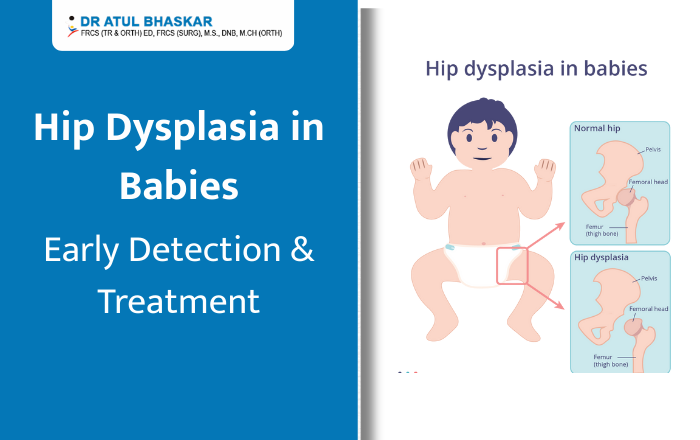
Hip Dysplasia in Babies: Early Identification & Treatment Guide for Parents
When you’re changing your baby’s diaper and notice one leg looks shorter than the other, or the skin folds don’t match up, it’s natural to feel worried. These could be early signs of hip dysplasia in babies—a condition where the hip joint doesn’t form properly. But here’s the good news: when spotted early, hip dysplasia is highly treatable. Most babies who receive timely care grow up to run, jump, and play just like other children. This guide will help you understand what to look for and when to seek help. What is Hip Dysplasia in Babies? Hip dysplasia in babies, also called Developmental Dysplasia of the Hip (DDH), happens when the hip joint doesn’t develop correctly. Think of a healthy hip as a ball sitting snugly in a socket. With hip dysplasia, the socket is too shallow, or the ball doesn’t fit properly. This can range from mild looseness to complete dislocation. About 1-2 babies per 1,000 are born with this condition. Girls are four times more likely to have it than boys. The condition can develop before birth, during delivery, or in the first year of life. 7 Warning Signs Every Parent Should Know Catching hip dysplasia early makes treatment easier. Watch for these signs during diaper changes: 1. Uneven skin folds – One thigh or buttock has more creases than the other 2. One leg looks shorter – When you bend both knees, one sits lower than the other 3. Limited hip movement – Difficulty spreading one leg to the side during diaper changes 4. Clicking sounds – You hear or feel a “clunk” when moving your baby’s legs 5. One foot turns out differently – The affected leg rotates outward more than the other 6. Uneven crawling or walking – Your child limps or favors one leg 7. Baby prefers one side – Doesn’t kick both legs equally or only rolls one direction Remember: Not all babies with hip dysplasia show obvious signs. This is why regular check-ups with your pediatrician matter. What Causes Hip Dysplasia? Several factors increase the risk of baby hip dysplasia: Breech position: Babies born bottom-first have higher risk Family history: Having a parent or sibling with hip dysplasia increases chances First-born babies: Less womb space can affect hip development Being female: Hormones make girls more susceptible Tight swaddling: Wrapping legs too straight can contribute to the problem You can help reduce risk by swaddling your baby with hips bent and free to move, and using baby carriers that support healthy hip positioning. How Doctors Check for Hip Dysplasia Your baby’s doctor will screen for hip dysplasia during regular visits. They’ll: Gently move your baby’s hips to check stability Look at leg length and skin folds Watch how your baby moves If something seems off, your doctor may recommend: Ultrasound (for babies under 6 months) – A safe, painless way to see the hip structure X-rays (for babies over 4-6 months) – Used once bones are more developed Studies show that early screening catches 90% of cases, leading to better results with simpler treatment. Treatment Options That Work The earlier hip dysplasia is found, the simpler the treatment. Here’s what to expect: ▸Pavlik Harness (For Babies Under 6 Months) This is the most common treatment. The soft harness holds your baby’s hips in the correct position for 6-12 weeks. Success rate? An impressive 90-95% when started early. Your baby can still move their legs and be held. Most parents say their little ones adjust within days. ▸Abduction Brace (For Older Babies) If your baby is over 6 months old, a stiffer brace might be needed. It keeps the legs in a “frog-leg” position and is worn for several months. ▸Closed Reduction If the harness doesn’t work, doctors can reposition the hip under anesthesia. Your baby will then wear a cast for 2-4 months. ▸Surgery (For Severe Cases) Reserved for complex situations or late diagnosis. With proper surgical treatment, children still have excellent long-term outcomes. ▸Will My Baby Walk Normally? Yes! With early treatment, over 95% of children with hip dysplasia lead completely normal, active lives. They participate fully in sports, dancing, and all childhood activities. Most children who wear a harness as infants show no lasting effects. You’d never know they had the condition. ▸Living with a Hip Harness Many parents worry about daily care, but it’s manageable: Diaper changes: Definitely possible—you’ll get the hang of it quickly Bathing: Your doctor will show you how to clean under the harness Sleep: Babies adapt fast and sleep comfortably Bonding: You can still cuddle, breastfeed, and comfort your baby normally When to See a Doctor Don’t wait if you notice: Any warning signs mentioned above Limping when your child starts walking Hip or leg pain in older children Any concerns about your baby’s hip development Hip dysplasia becomes harder to treat the longer it goes undiagnosed. Trust your instincts—if something feels wrong, get it checked. Get the Right Care in Mumbai If you’ve noticed signs of hip dysplasia in your baby, or your child has been diagnosed, getting proper medical care is crucial. Dr. Atul Bhaskar, a Paediatric Orthopaedic Surgeon in Mumbai, specializes in treating hip dysplasia and other childhood conditions. With extensive experience in both harness treatment and surgical options when needed, Dr. Bhaskar helps families navigate this journey with confidence. Why families choose Dr. Atul Bhaskar: Specialized training in children’s hip conditions Experience with Pavlik harness fitting and monitoring Surgical expertise for complex cases Clear explanations that parents understand Supportive care throughout your child’s growth Your baby’s hip health is important. Early diagnosis and proper treatment mean your little one can grow up healthy, active, and pain-free. Schedule a consultation with Dr. Atul Bhaskar today to get the answers and treatment your family needs.
Shoulder Dislocation in Kids: Causes, Symptoms, and Recovery Timeline
Shoulder Dislocation in Kids: Causes, Symptoms, and Recovery Timeline When your child suddenly grabs their shoulder in pain during a game or after a fall, your heart skips a beat. Is it serious? What should you do? If you’re searching for answers about shoulder dislocation in kids, you’re in the right place. Shoulder dislocations can happen to children, especially active ones who love sports and outdoor play. While it’s more common in teenagers than younger kids, knowing what to look for and how to respond can make all the difference. Let’s break down everything you need to know in simple terms. What Is a Shoulder Dislocation? Think of your child’s shoulder as a ball sitting in a shallow cup. The upper arm bone (the ball) normally sits snugly in the shoulder socket (the cup). A dislocation happens when that ball pops completely out of the socket. This is different from a shoulder separation, which affects a different part of the shoulder where the collarbone meets the shoulder blade. It’s also more serious than a strain or sprain. Children’s shoulders are still growing, which actually makes complete dislocations less common in younger kids compared to teens. Their bones and joints are more flexible, but when a dislocation does happen, it needs immediate medical attention. What Causes Shoulder Dislocation in Children? Sports InjuriesMost shoulder dislocations in kids happen during sports, especially: Contact sports like football, hockey, or rugby Activities with potential falls like gymnastics or wrestling Overhead sports such as swimming, baseball, or volleyball A direct hit, awkward landing, or extreme arm movement can force the shoulder out of place. Falls and Accidents Outside of sports, common causes include: Playground accidents and falls Bicycle or skateboard crashes Landing on an outstretched arm during play Car accidents (less common but possible) Joint LoosenessSome children have naturally looser joints, making dislocations more likely. This can run in families or be part of certain medical conditions affecting connective tissue. How to Tell If Your Child’s Shoulder Is Dislocated Look for These Signs: ▹Pain and Position Sudden, intense pain in the shoulder Your child can’t move their arm They hold their arm in an odd position away from their body They may tell you something “popped out” ▹Visible Changes The shoulder looks different or deformed One shoulder appears lower than the other Swelling develops quickly Bruising may appear Important: Never try to put the shoulder back in place yourself. This can cause more damage to nerves, blood vessels, and soft tissues around the joint. When to Get Help A dislocated shoulder always requires immediate medical care. Take your child to the emergency room right away. The doctor needs to examine the injury, take X-rays, and properly relocate the shoulder joint. How Doctors Treat Shoulder Dislocation ▹ Putting the Shoulder BackThe medical term is “reduction,” but it simply means the doctor carefully moves the arm bone back into the shoulder socket. For children, doctors usually give medicine to help them relax or sleep during this procedure because it can be uncomfortable. ▹Rest and ProtectionAfter the shoulder is back in place, your child will wear a sling for about 2 to 4 weeks. This keeps the shoulder still so it can heal properly. The doctor will also recommend: Ice packs to reduce swelling (15-20 minutes at a time) Pain medicine safe for children Keeping the arm supported and rested Surgery—When Is It Needed? Most children don’t need surgery for a first-time dislocation. However, surgery might be necessary if: The shoulder keeps dislocating repeatedly There’s a fracture along with the dislocation Soft tissues are badly damaged The child is a teenager active in competitive sports The Recovery Timeline ▹Weeks 1-2: Rest and HealingYour child wears the sling constantly and avoids moving the shoulder. Focus on comfort and pain management during this time. ▹Weeks 3-6: Gentle MovementThe doctor may start gentle exercises to restore movement. Physical therapy often begins here, with simple exercises your child can do at home. ▹Weeks 6-12: Building StrengthExercises become more active, focusing on strengthening the muscles around the shoulder. This phase is crucial for preventing future dislocations. ▹Months 3-6: Return to PlayMost kids can gradually return to sports and activities during this period, but always with their doctor’s approval. Contact sports usually require the longest wait. Remember, every child heals differently. Your doctor will guide you based on your child’s specific situation. Preventing Future Shoulder Problems Once a shoulder dislocates, there’s a higher chance it could happen again, especially in teenagers. Here’s how to reduce that risk: Complete all physical therapy exercises as recommended Strengthen shoulder muscles regularly Use proper technique in sports Wear protective gear when appropriate Warm up before activities Don’t rush back to sports too soon When to See a Shoulder Specialist If your child has dislocated their shoulder or you’re worried about shoulder instability, seeing an experienced orthopedic doctor is important. The right treatment now can prevent ongoing problems later. Dr. Atul Bhaskar has over 33+ years of experience treating shoulder injuries, including shoulder dislocation treatment in Mumbai. With extensive knowledge in pediatric shoulder care, Dr. Bhaskar understands how to treat young patients while considering their growth and active lifestyles. From diagnosis through complete recovery, Dr. Bhaskar focuses on getting children safely back to their favorite activities while protecting their long-term shoulder health. Don’t wait if your child is experiencing shoulder problems. Schedule a consultation to discuss your child’s shoulder health and the best treatment options for their needs. Contact Dr. Atul Bhaskar today for shoulder dislocation treatment in Mumbai and help your child get back to doing what they love.
Pigeon Toes in Children: What Causes In-Toeing and How to Treat It
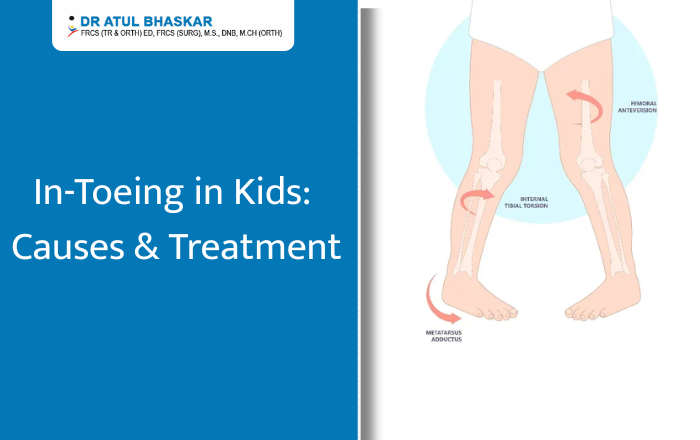
Pigeon Toes in Children: What Causes In-Toeing and How to Treat It Have you noticed your child walking or running with their feet pointing inward? This is known as pigeon toes or in-toeing, and it’s a common concern among parents. While it can look unusual, in many cases it’s simply a part of your child’s growth pattern and improves with time. However, sometimes it can be a sign that your child needs help to correct their walking style. In this blog, we’ll explain what pigeon toes are, what causes them, when to be concerned, and the different treatment options available. We’ll also share some home tips that may help your child’s feet grow in the right direction. What Are Pigeon Toes (In-Toeing)? Pigeon toes describe a walking pattern where a child’s feet point inward instead of straight ahead. This can happen in one foot or both. Parents usually notice it when their child starts walking, but it can also appear later in early school years. While it often corrects naturally, persistent or severe in-toeing should be checked by a doctor. Common Causes of In-Toeing in Children 1. Metatarsus AdductusThis condition appears in babies when the front part of the foot curves inward. It can happen because of the baby’s position in the womb. Mild cases often improve on their own, but stretching exercises may be suggested for some children. 2. Tibial TorsionIn toddlers, in-toeing can happen when the shinbone (tibia) naturally twists inward. This usually becomes noticeable when the child begins walking. As the child grows, the tibia often straightens out without treatment. 3. Femoral AnteversionThis occurs when the thigh bone (femur) twists inward, making the knees and feet turn in. It’s often most noticeable between ages 3 and 8. Many children grow out of it, but in some cases, it continues into later childhood. 4. Genetic and Developmental FactorsSome children have a family history of in-toeing. Growth patterns, sitting posture, and early walking habits can also influence how the feet and legs align. Symptoms and When to Seek Medical Advice Mild in-toeing is usually harmless. However, you should see a doctor if: Your child often trips or falls. The condition worsens over time. There is pain, limping, or swelling. One leg or foot looks very different from the other. Diagnosis: How Doctors Evaluate In-Toeing A pediatric orthopedic doctor will: Ask about your child’s growth and walking habits. Check leg and foot alignment during a physical exam. Observe your child’s gait while walking or running. Use X-rays or scans if needed to understand bone position. Treatment Options for Pigeon Toes 1. Observation and Natural CorrectionMost cases improve naturally as the bones and muscles develop. Doctors often recommend regular monitoring to track changes. 2. Stretching and ExercisesSpecific exercises can help improve muscle strength and foot alignment. These may include balance games, stretching routines, and walking on different surfaces. 3. Orthotics and Supportive FootwearIn some cases, special shoe inserts or braces are suggested to guide foot position. These are usually for children with more persistent symptoms. 4. Medical or Surgical InterventionSurgery is rarely needed, but in severe cases where in-toeing affects mobility or daily activities, it may be considered. Home Care and Prevention Tips Encourage barefoot walking indoors on safe, flat surfaces. Avoid letting your child sit in the “W” position. Include outdoor play and activities that strengthen leg and foot muscles. Make walking and balance games part of daily fun. Possible Complications if Left Untreated While many children experience no issues, untreated severe in-toeing can lead to: Frequent tripping or falling. Difficulty in sports or running. Increased strain on knees and hips over time. When to See a Pediatric Orthopedic Specialist You should consider a specialist if: Your child’s in-toeing persists beyond age 8. Pain or discomfort is present. The condition is affecting confidence or physical activities. Help Your Child Walk Confidently – Book a Consultation Today Most cases of pigeon toes in children are simply a stage of growth. Still, it’s always best to keep an eye on your child’s walking style and get professional advice if you notice ongoing problems. If you are concerned about your child’s in-toeing or walking pattern, don’t wait for it to worsen.For proper evaluation and treatment, you can consult Dr. Atul Bhaskar – Pediatric Orthopedic Surgeon in Mumbai. FAQ Q1: Is pigeon toe normal in toddlers?Yes, many toddlers have in-toeing, and it often improves naturally with age. Q2: Can pigeon toes cause problems later in life?Mild cases usually cause no issues, but severe cases may lead to tripping or joint strain. Q3: How can I help correct my child’s in-toeing at home?Encourage barefoot walking on safe surfaces, avoid W-sitting, and include balance activities in playtime.

Cast vs. Splint for Child Fractures: What’s the Right Option?
Cast vs. Splint for Child Fractures: What’s the Right Option? When your child gets hurt, especially if it might be a broken bone, it’s stressful. One of the first questions that comes up is whether they need a cast or a splint. It’s not always easy to tell which is better—and most parents just want to do the right thing as quickly as possible. This article will walk you through the difference between a cast and a splint, how doctors decide between them, what healing looks like, and what parents need to know to make smart choices. Let’s break it down in simple terms. What Happens When a Child Breaks a Bone Why Fractures Are Common in Kids Kids are active. They climb, run, fall, and bounce right back up—most of the time. But growing bones are softer than adult bones, so they break more easily. A small trip or a fall from a swing can lead to a fracture. Common fracture spots in children include: Wrist (from trying to break a fall) Elbow (especially from monkey bars) Forearm or collarbone (during sports or rough play) Signs Your Child Might Have a Fracture Swelling or bruising that gets worse Pain when moving the arm or leg A limb that looks bent or different Refusing to move the injured part Crying even after some time has passed If any of these signs are there, it’s best to see a pediatric orthopedic doctor right away. Cast vs. Splint: What’s the Real Difference? Both casts and splints are used to keep a broken bone in place so it can heal. But they’re not the same thing. What Is a Cast? A cast is a hard shell made from fiberglass or plaster. It wraps around the limb completely and holds the bone steady. When casts are used: For serious or unstable fractures When the bone needs to stay in one exact position For longer healing time Pros: Very strong and stable Can’t be removed by the child Cons: Heavy Can’t get wet Might feel tight as swelling goes down Needs a special tool to remove What Is a Splint? A splint is sometimes called a half-cast. It supports only one side of the limb and is held on with bandages or Velcro. When splints are used: For small or hairline fractures When swelling is still happening As a first step before a cast Pros: Easier to adjust Lighter and more comfortable Can be removed for cleaning or checking (if the doctor allows) Cons: Not as firm as a cast Can shift if not worn properly Some kids may try to remove it on their own How Doctors Decide: Cast or Splint? The choice between a cast and a splint isn’t random. Doctors look at a few key things: How bad the break is Where the bone is broken How much the bone has moved The child’s age and activity level If swelling is still present Example:A small crack in the wrist might heal well with a splint. But a full break near the elbow probably needs a cast to keep the joint stable. Healing Time: What Parents Should Know How Long Does It Take to Heal? It depends on the break. But in most cases: Minor fractures: 3 to 4 weeks Moderate to serious fractures: 6 to 8 weeks Near a joint or growth plate: Sometimes longer, with closer follow-up Kids heal faster than adults, but they also need more careful checks because their bones are still growing. Caring for a Cast or Splint at Home Tips: Don’t get it wet (unless your doctor says waterproof is okay) Keep the limb raised in the first few days to reduce swelling Check fingers or toes for color, warmth, and movement Don’t stick anything inside to scratch Tell the doctor if it smells bad, feels too tight, or causes more pain Cast vs. Splint: Which One Is Better for Your Child? There’s no clear “better” option it all comes down to what the injury needs. Condition Cast Splint Full bone break ✅ Yes ❌ No Minor crack ❌ Not always needed ✅ Often enough Swelling present ❌ Not ideal at first ✅ Gives room to adjust Long-term healing needed ✅ Strong and secure ❌ Usually temporary If you’re unsure, don’t guess—ask a pediatric orthopedic doctor who works with kids regularly. FAQs Q: Is a splint strong enough for a broken bone?It can be, if the break is small or hasn’t shifted. Doctors often use splints first, then switch to a cast once swelling goes down. Q: Can my child take off the splint at home?Only if the doctor says so. Some splints are made to be removable. Others aren’t. Q: Will my child need physical therapy after the cast or splint?Not always. Most kids bounce back fast. But if movement is stiff after healing, therapy might help. Choosing between a cast or a splint isn’t just about comfort—it’s about healing the right way. The best choice depends on the type of fracture, the child’s age, and how their bones are growing. Always follow the advice of a pediatric orthopedic specialist who understands how children heal. Need Help Deciding What’s Right for Your Child? If your child has a broken bone or you’re unsure what kind of treatment they need, don’t wait and wonder. Reach out to Dr. Atul R. Bhaskar, a trusted Pediatric Orthopedic Doctor in Mumbai with 33+ years of experience helping children recover from fractures and other bone injuries. He has treated thousands of kids with care, skill, and the kind of calm that reassures both parents and little ones.
Leg Length Discrepancy in Children: Causes and Treatments
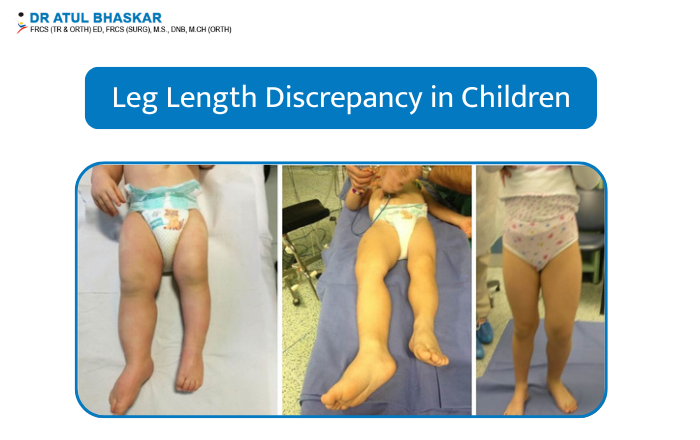
Have you noticed your child walking with a limp or uneven step? Does one leg seem shorter than the other? These could be signs of leg length discrepancy (LLD)—a condition where one leg is slightly or significantly shorter than the other. This condition can affect a child’s balance, walking pattern, and even their posture if not managed early. In this blog, we’ll explore what causes uneven leg length in children, how it’s diagnosed, and the most effective treatment options for leg length discrepancy in kids. We’ll also share when surgery might be needed and how to support your child through it. What Is Leg Length Discrepancy in Children? Leg length discrepancy happens when there is a noticeable difference in the lengths of a child’s legs. It may be small (a few millimeters) or more significant (several centimeters). There are two types: Structural discrepancy – A true difference in bone length. Functional discrepancy – Legs may be the same length, but something like a hip or spine issue makes them appear uneven. Some kids might not have any pain, while others may struggle with walking, balance, or discomfort in the lower back and knees. What Causes Uneven Leg Length in Children? There are several reasons why one leg may grow longer or shorter than the other: Congenital issues – A child may be born with a shorter leg due to how the bones developed in the womb. Injuries – Damage to the growth plate from a fracture can slow down or stop growth in one leg. Bone infections – Certain infections during childhood can affect bone growth. Neurological conditions – Disorders like cerebral palsy can impact muscle tone and posture, causing the legs to appear different in length. Tumors or cysts – Rarely, these can affect bone growth. Previous surgeries – Some operations may influence the way a leg grows. If you’re wondering about the common causes of leg length discrepancy in kids, it’s important to understand that most cases develop over time and can be noticed gradually. Signs and Symptoms to Look Out For Here are some common signs that may suggest your child has a leg length difference: Limping or favoring one leg One shoe wearing out faster than the other Complaints of hip, knee, or back pain Trouble running or keeping up with other kids Tilting or leaning to one side while standing or walking Parents often ask how to identify leg length discrepancy in a child—if you notice even slight differences, it’s a good idea to talk to a pediatric orthopedic specialist. How Is Leg Length Discrepancy Diagnosed in Children? Diagnosing LLD involves both a physical check-up and imaging tests. Here’s what usually happens: Physical exam – A doctor will look at how your child walks, stands, and moves. Measuring tools – Leg lengths are measured to find out the difference. X-rays or EOS scans – These give detailed images of the bones and help measure any discrepancy more accurately. Gait analysis – Helps doctors see how the legs and feet move during walking. A pediatric diagnosis of leg length discrepancy is usually clear once the imaging is done. Treatment Options for Leg Length Discrepancy in Children Not all cases need treatment right away. The best option depends on your child’s age, the amount of difference, and how it affects their daily life. ObservationIf the difference is small (less than 2 cm), doctors may simply monitor it over time to see how it changes as your child grows. Shoe Lifts or OrthoticsThese are used to balance the leg length difference and help your child walk more evenly. Surgical Treatments If the difference is larger or causing problems, surgery may be recommended: Epiphysiodesis – A procedure that slows growth in the longer leg, allowing the shorter leg to catch up. Leg lengthening – A special frame or device is used to slowly stretch the shorter bone and help it grow over time. Treatment for mild and severe leg length discrepancy in children is chosen based on how much the difference affects movement and comfort. When Is Surgery Needed for Uneven Leg Length in Kids? Surgery is usually considered when the difference is expected to be more than 2–5 cm at maturity or if your child has trouble walking or pain. Surgery May Be Needed If: There is a large projected difference in leg length Walking is difficult or painful Shoe lifts are not helping enough After surgery, physical therapy and regular follow-ups help with recovery. Leg lengthening surgery for children is done in stages and may take several months to complete. Why Early Treatment Matters: Preventing Long-Term Problems Ignoring leg length differences can lead to more serious problems later: Back pain and posture issues Uneven hips or pelvis Joint stress in knees or ankles Difficulty keeping up in physical activities Long-term effects of untreated leg length discrepancy in kids can be avoided with timely treatment and follow-up. Meet the Doctor: Dr. Atul Bhaskar – Pediatric Orthopedic Surgeon in Mumbai If you’re looking for someone with deep experience in managing leg length issues in children, Dr. Atul Bhaskar is a trusted name in pediatric orthopedic in Mumbai. He treats children with leg length discrepancies using both non-surgical and surgical methods, based on what’s right for each child’s situation. Parents across Mumbai consult him for conditions like flat feet, hip problems, and growth disorders in kids. To schedule a consultation, you can visit his clinic or get in touch online. Long-tail keyword suggestion: best pediatric orthopedic doctor in Mumbai for leg length discrepancy Frequently Asked Questions 1. What is a normal leg length difference in children?A small difference (less than 1 cm) is usually harmless. Larger differences may need treatment. 2. Can leg length discrepancy fix itself over time?Minor differences might not get worse and sometimes even out as a child grows. Regular monitoring is important. 3. What are the non-surgical treatment options?Shoe lifts, physiotherapy, and regular check-ups are used for smaller discrepancies. Take the First Step Toward Your